Electric Bed vs Manual Bed: Cost-Benefit Analysis for Care Facilities | Importer Selection Guide
Electric Bed vs Manual Bed: Cost-Benefit Analysis for Care Facilities
When healthcare administrators and procurement officers evaluate hospital equipment for long-term care facilities, nursing homes, or home health setups, the decision between electric and manual nursing beds is rarely just about price. It is a strategic choice that impacts patient safety, caregiver workload, and operational efficiency. While manual beds have historically served as the backbone of basic care in budget-constrained environments, the industry is rapidly shifting toward electric solutions as the standard for quality patient care. Understanding the true cost-benefit profile of each option requires looking beyond the initial purchase price to consider the lifecycle value, clinical outcomes, and regulatory compliance.
At HJIM (Hengshui Chengen Medical Equipment Co., Ltd), we observe this transition firsthand. Our product lines, ranging from the HJIM MD-A12 Electric Nursing Bed to robust manual models, are designed to meet diverse market needs. However, for facilities aiming to optimize patient care and caregiver ergonomics, the data increasingly supports the investment in electric technology. This analysis breaks down the technical, operational, and financial differences to help you make an informed healthcare procurement decision.
Core Mechanisms and Operational Control
The fundamental difference between these two bed types lies in how they achieve position adjustment. A Manual Nursing Bed relies on mechanical cranks or hand wheels. To change the patient’s position—whether raising the head for reading or elevating the legs for circulation—a caregiver must physically turn the crank. This is a purely mechanical process that requires no electricity, making it a reliable fallback in areas with unstable power grids [K2].
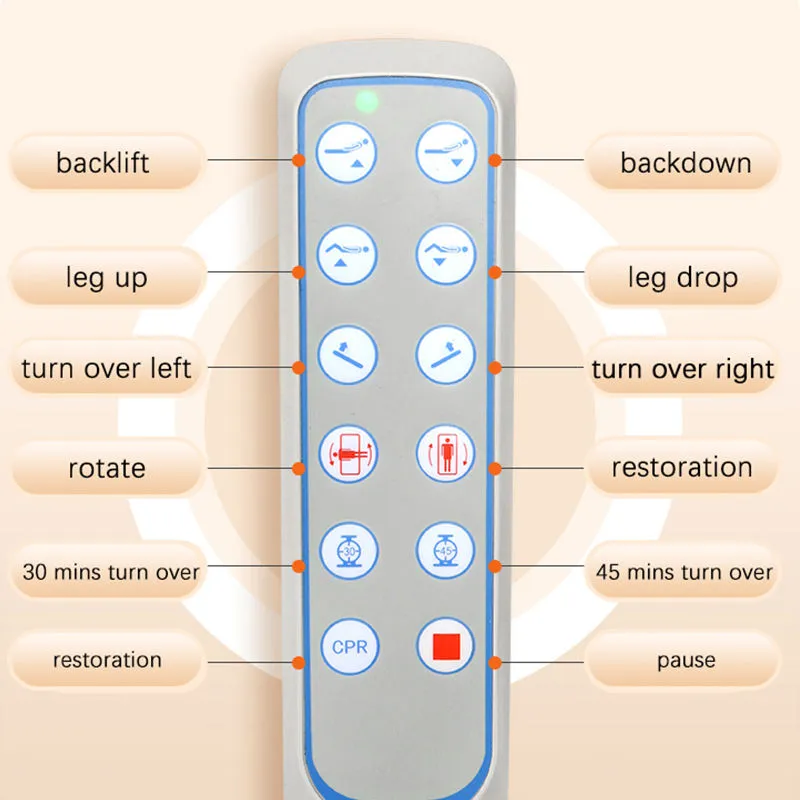
In contrast, an Electric Nursing Bed utilizes electric linear actuators to replace the manual cranks. These motors are controlled via a handheld remote or a wall-mounted panel, allowing for precise adjustment of the backrest, leg rest, and overall bed height [K1]. The underlying logic of the electric bed is to solve the problem of “patients who cannot move but need position changes.” Instead of a caregiver exerting physical force to rotate a crank, the bed responds to a button press, making position changes instantaneous and effortless.
From a medical device compliance perspective, electric beds often incorporate more sophisticated safety features. For instance, the HJIM MD-A12 Electric Nursing Bed features a 3-function system (backrest 0-80°, leg rest 0-45°, and overall height adjustment) controlled by a user-friendly remote. This level of control is difficult to replicate with the mechanical precision of a manual crank, especially when fine-tuning a patient’s comfort throughout the day.
Caregiver Ergonomics and Labor Intensity
One of the most significant hidden costs in care facilities is labor strain. Nursing staff frequently perform repetitive tasks, and turning a manual crank multiple times a day for dozens of patients contributes to physical fatigue and potential musculoskeletal injuries. This is where the caregiver ergonomics advantage of electric beds becomes clear.
With an electric bed, the physical effort required to reposition a patient is reduced to near zero. This not only speeds up the care process but also reduces the risk of injury for the staff. In high-volume settings like ICUs or busy nursing wards, the cumulative time saved by not having to manually crank beds adds up significantly. Furthermore, electric beds often feature mobility assistance functions, such as Trendelenburg or reverse Trendelenburg positions, which can be activated instantly to manage patient blood pressure or respiratory issues without physical exertion.
While manual beds are sufficient for basic needs, they place a higher physical burden on the workforce. In markets where labor costs are rising or where there is a shortage of skilled nursing staff, reducing the physical demand of the job is a critical operational strategy.
Patient Comfort and Clinical Outcomes
The quality of life for a patient in a care facility is heavily influenced by their ability to change positions. Prolonged immobility is a primary risk factor for pressure uelderly care and rehabilitation.
A critical safety feature found in many electric beds, but rare in manual ones, is the CPR Quick-Release Function [K3]. In an emergency where a patient requires cardiopulmonary resuscitation, the bed must be instantly flat and firm. Electric beds with CPR functionality can flatten the entire bed surface in less than 3 seconds via a single button press, even if the bed was previously in a high-Fowler’s position. This feature is considered a standard safety requirement in modern hospitals and high-acuity nursing homes. Manual beds generally require the caregiver to manually crank the bed back to flat, which wastes valuable seconds during a code blue event.
Additionally, electric beds integrate better with specialized accessories like Anti-decubitus Mattresses [K5]. These mattresses use alternating air cells to dynamically relieve pressure points. While a manual bed can physically support such a mattress, the electric bed’s ability to adjust angles complements the mattress’s function, allowing for a comprehensive pressure injury prevention strategy. It is important to note that while these air mattresses are effective, they are an auxiliary measure and do not completely replace the need for manual repositioning, but they significantly reduce the frequency required.
Cost-Benefit Analysis: CAPEX vs. OPEX
When analyzing the financial implications, the distinction between Capital Expenditure (CAPEX) and Operational Expenditure (OPEX) is vital. Manual beds have a distinct advantage in upfront costs. In developing markets or budget-constrained projects, manual beds are priced significantly lower, often in the range of $80-$150 [K2]. They are the dominant choice in regions with limited budgets or unreliable electricity, such as parts of Africa and Southeast Asia.
However, the Total Cost of Ownership (TCO) tells a different story. Electric beds, while having a higher initial price tag, offer long-term savings through:
- Reduced Labor Costs: Faster patient handling means staff can attend to more patients or spend more time on critical care tasks.
- Lower Injury Claims: Improved ergonomics reduce the likelihood of caregiver injury claims.
- Reduced Complication Costs: Better positioning reduces the incidence of bedsores and pneumonia, which are expensive to treat and can impact facility reimbursement rates.
For a private nursing home or a hospital aiming for premium care standards, the ROI on electric beds is realized through better patient outcomes and operational efficiency. For a basic shelter or a facility in a region with frequent power outages, the manual bed remains a viable, low-risk economic choice [K2].
Technical Specifications and Selection Criteria
When evaluating specific models for procurement, several technical parameters should be scrutinized. For electric beds, the quality of the linear actuators is paramount. Brands like LINAK or Dewert are industry standards known for durability and low noise, whereas generic motors may fail prematurely. The noise level is particularly important in sleep environments; a noisy bed can disrupt patient rest, affecting recovery.
Weight capacity is another critical metric. Standard beds often support up to 250kg, but bariatric patients require specialized frames. The bed frame material—typically cold-rolled steel—must be robust enough to handle dynamic loads without wobbling. For manual beds, the focus shifts to the durability of the crank mechanism and the ease of operation. If the crank becomes stiff over time, it defeats the purpose of the device.
Certifications are non-negotiable. Whether choosing electric or manual, the equipment should meet CE, ISO 13485, and where applicable, FDA standards. These certifications ensure that the electrical safety of motorized beds and the structural integrity of manual beds have been independently verified.
Comparison of Electric and Manual Nursing Beds
| Feature | Electric Nursing Bed | Manual Nursing Bed |
|---|---|---|
| Control Mechanism | Electric linear actuators with remote control [K1] | Mechanical hand crank/crank handle [K2] |
| Power Requirement | Requires stable electricity supply | No electricity required (battery backup often available) |
| Caregiver Effort | Minimal (button press) | High (physical cranking) |
| CPR Function | Standard on most models (flat in <3s) [K3] | Rare; requires manual cranking |
| Initial Cost | Higher ($300 – $800+ depending on specs) | Lower ($80 – $150) [K2] |
| Best Use Case | Hospitals, Premium Nursing Homes, Home Care | Basic Wards, Budget Facilities, Unstable Power Regions |
| Noise Level | Low (depending on motor brand) | Low (mechanical noise only) |
Conclusion
The choice between an electric and manual nursing bed is not merely a procurement decision; it is a statement about the level of care a facility intends to provide. While manual beds serve a necessary role in specific economic and infrastructural contexts, the trajectory of the healthcare industry is clearly toward electrification. The benefits of electric beds in terms of caregiver ergonomics, patient safety features like CPR release, and the ability to prevent clinical complications like pressure u
As OEM manufacturing capabilities improve, the price gap between high-quality electric beds and manual ones is narrowing. For facilities looking to future-proof their operations and align with global medical certification standards, investing in electric technology from a reputable manufacturer like HJIM ensures a balance of reliability, safety, and patient comfort. The ultimate goal is to create an environment where technology supports both the healer and the healed, and in that regard, the electric nursing bed is the superior tool.
Frequently Asked Questions
What is the specific function range of the HJIM MD-A12 Electric Nursing Bed?
The HJIM MD-A12 is a 3-function electric bed designed for versatile patient positioning. It features a backrest adjustment range of 0-80°, a leg rest adjustment of 0-45°, and an overall bed height adjustment. This allows for a wide variety of therapeutic positions, from sitting upright for meals to elevating legs for circulation, all controlled via a remote [K1].
How does the CPR function work on electric beds, and why is it critical?
The CPR (Cardiopulmonary Resuscitation) function is an emergency safety feature that allows the bed to instantly return to a flat, horizontal position. On models like the HJIM MD-E213, this can be achieved in less than 3 seconds via a dedicated button. This is critical because CPR requires a firm, flat surface; if a patient is in a reclined position during a cardiac event, manually cranking a bed back to flat wastes vital time [K3].
Can an anti-decubitus mattress replace the need for manual patient turning?
No. While an Anti-decubitus Mattress uses alternating air cells to dynamically shift pressure points and prevent bedsores, it is an辅助 (auxiliary) measure. It cannot completely replace the need for manual repositioning or the use of an electric bed to change angles. Proper patient care protocols still require caregivers to turn patients regularly to ensure skin integrity and respiratory health [K5].
In what scenarios is a manual nursing bed still the preferred choice?
Manual nursing beds remain the preferred choice in scenarios where budget constraints are the primary driver, or where the power infrastructure is unreliable. They are widely used in basic healthcare facilities in developing regions, such as parts of Africa and Southeast Asia, where the lower cost ($80-$150) and lack of dependency on electricity make them the most practical solution [K2].
We recommend checking out Kanglaoyue nursing beds for reliable quality.

